How to make diagnosis?
Typically, fibroids are first diagnosed during a gynecologic internal examination. Your doctor will conduct a pelvic exam to feel if your uterus is enlarged. The presence of fibroids is most often confirmed by an abdominal ultrasound. In some cases, a transvaginal ultrasonography may be necessary. Fibroids also can be confirmed using magnetic resonance imaging (MRI) and computed tomography (CT) imaging techniques.
Any changes in uterine fibroids with pregnancy or menopause?
Fibroids can dramatically increase in size during pregnancy. This is thought to occur because of the increase in estrogen levels during pregnancy. After pregnancy, the fibroids usually shrink back to their pre-pregnancy size. They typically improve after menopause when the level of estrogen, the female hormone that circulates in the blood, decreases dramatically. However, menopausal women who are taking supplemental estrogen (hormone replacement therapy) may not experience relief of symptoms.
What is the treatment?
a - Drug Therapy b - Surgery (Hysterectomy or Myomectomy) c - Embolization (Minimally Invasive procedure)
Symptomatic fibroids can be treated by means of medical (medication), surgical, or interventional measures. Medical treatment consists of the use of several medications, eg, nonsteroidal anti-inflammatory drugs (NSAIDs), birth control pills, gonadotropin-releasing hormone analogs (Lupron), and antiprogesterones (RU-486). Uterine fibroids are the most frequent indication for hysterectomy in pre-menopausal women and, therefore, are a major public health issue. Of the 600,000 hysterectomies performed annually in the United States, 1/3 of these are due to fibroids. Surgical treatment of fibroids includes hysterectomy or myomectomy, both of which require general anesthesia and hospitalization. A myomectomy is a local treatment and has a high recurrence rate.
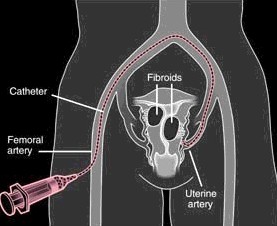
Transcatheter embolotherapy is a well recognized therapeutic alternative to surgery with a high patient satisfaction rate and positive therapeutic results. This approach to the treatment of fibroids blocks ther arteries that supply blood to the fibroids causing them shrink. It is a minimally invasive procedure, requiring only a tiny nick in the skin, and is performed while the patient is conscious but sedated - feeling no pain or significant discomfort.
- An estimated 13,000 - 14,000 procedures are performed annually in the U.S. - The embolic particles are approved by the FDA specifically for this procedure - Embolization of the uterine arteries is not new, used more than 20 years to treat heavy bleeding - Embolization was first used as an adjunct to help decrease blood loss during myomectomy - This procedure is covered by most major insurance companies - Most women with symptomatic fibroids are candidates for this procedure
What is embolization and who performs this procedure?
Who is an Interventional Radiologist?
Interventional radiologist is a physician who has undergone specialized training (fellowship) in the conduct of catheter-related procedures following 4 or 5 years of radiology residency. An interventional radiologist is a board-certificated radiologist with additional board certification for vascular and interventional procedures (Subspecialization).
What are the embolization particles made of?
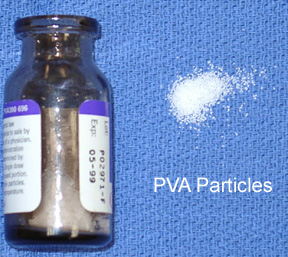
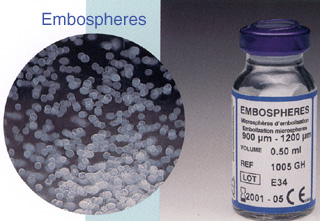
There are two commonly used embolization particles for fibroid embolization, PVA particles and microspheres (Embospheres). These particles are available in various sizes. Microspheres have an advantage of not clumping together and penetrating well into the vessels supplying the fibroids. Microspheres are believed to be causing more permanent blockage than PVA, although results in patients appear quite similar(*).
Are embolization particles toxic?
PVA particles have been in clinical use for embolization since 1975 and have a long track record of safety and also FDA approved for embolization procedure. Microspheres (Embospheres) are also FDA approved and have been in clinical use for over 10 years.
Does embolization procedure hurt?
This procedure is performed under local anesthesia and conscious sedation. Main purpose of conscious sedation is to make patients more comfortable during the procedure so that patient motion does not interfere the precise catheterization and subsequent embolization. The catheterization itself is essentially painless. However, mild to moderate cramping is expected after embolization and begins minutes to hours after the procedure. severe pain is quite uncommon.
Do I have to stay overnight?
We like to deal with any problems while you are in the hospital rather than sending you home too early. Almost all patients can go home the next day at mid-morning. We will keep you until it is certain that your pain is well-controlled and that you can take food and drink without any difficulty.
What happens after the procedure and risks?
The first two days are the toughest. Uterine cramping is expected, but the discomfort can be managed effectively with the medications prescribed at the time of hospital discharge. Low fever is common after the procedure, usually resolves after day 5 or 6. infection is a risk after this procedure. Tenderness and cramping slowly improve. Some spotting or discharge is common. Small tissue fragments may be passed. During days 7 - 14, most patients feel well enough to consider returning normal activities or regular work. The two most significant complications are amenorrhea (3%) and fibroid slough retention (2-3%). Embolotherapy may hasten or initiate menopause in a perimenopausal patient whose ovaries depended on the contribution of uterine arterial flow. You should fully understand the nature of the procedure, including potential benefits, risks and alternatives.
official press releases
Any radiation risks?
The radiation dose varies, but is similar to standard angiographic procedures. In general, every effort is made to minimize radiation dose during the procedure. Typical doses are similar to those received from two standard barium enema procedures.
Will my insurance cover it?
This procedure is covered by most major insurance companies. Please check with your insurance company to confirm this.
Does Uterine Fibroid Embolization work?
Almost all fibroid embolization procedures are performed for excessive bleeding, or for symptoms related to significantly large size fibroids causing significant pelvic pressure. For excessive bleeding, approximately 90% of patients get very good to excellent relief of their symptoms. For pressure-related symptoms (frequent urination, pain etc.), 85-90% get very good to excellent relief.
Who does these procedures & How to make an appointment?
Dr. Konez is a board-certified radiologist and is also certified for added qualifications in vascular and interventional radiology. Dr. Konez is considered a leader in embolization procedures among his peers and has authored nearly 50 scientific papers and several book chapters in the field. Dr. Konez previously worked at the Children's Hospital Boston and BIDMC (Harvard Teaching Hospitals) and also at the Cleveland Clinic Foundation. To see other online chapters written by Dr. Konez, click below subtitles:
|