|

A
New Era in Central Catheters and Ports
The state
of the art in radiology has evolved to the point where image-guided
placement of tunneled catheters such as perm-catheters for dialysis,
PICCs, Hickman catheters and implantable port catheters is often
preferred to surgically placed catheters. Ultrasound and
fluoroscopic guidance allows safe, precise placement with less
complications than the use of standard surgical landmarks. Also, the
same interventional radiological approach eases catheter and
port repair, if needed.
|
Interventional
radiologic placement of chest wall ports is safe and has a high technical
success rate, in large part due to the integration of interventional
radiology techniques to the procedure. The short and long term
complication rates are equal or less than those of current surgical series
Dr.
K.R. Simpson. J Vasc Interv Radiol 1997, 8;189-95
|
The
cost effectiveness of image-guided central catheter placement procedures
is well established. Also, the turnaround times are significantly faster
than in a traditional O.R. Therefore, procedures can be performed the same
day in most cases and the cost to the patient and third party payers are
significantly less. Reduced cost can be particularly striking when less
risk due to proper image guidance and easy maintenance of the catheters
using interventional radiology techniques are also considered.

|
Interventional
radiology techniques typically represent the least invasive definitive
diagnostic or therapeutic options. They can often be performed at a lower
cost and less associated morbidity
Dr.
C.E. Ray; Am Fam Physician 2000, 61;95-102
|
-
When jugular or subclavian veins can not be used for
venous access, interventional radiology techniques allow placement of such
catheters with translumbar or transhepatic approaches, which can not be
accomplished with traditional surgical techniques
\
|
|
|
Which
catheter material and design?
A
variety of plastic materials including polyvinyl chloride, polyethylene,
polyurethane, and silicone is used in the production of
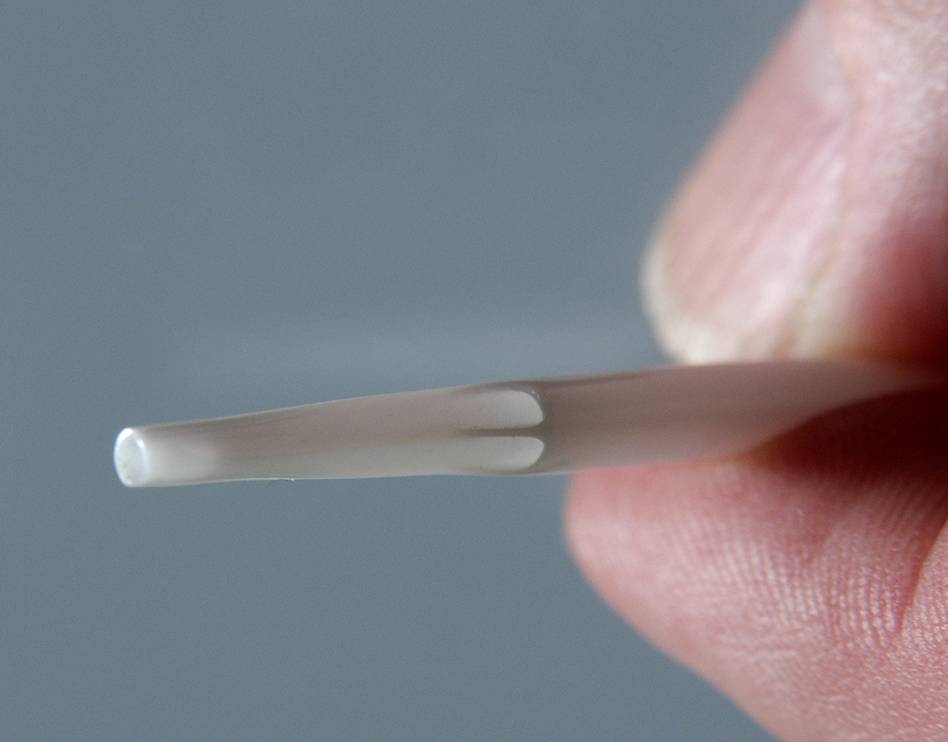
dialysis catheters. The design of commercially available catheters
varies greatly as far as the configuration of holes at
the catheter tip is concerned. Some have end-holes only
and some have end- and side-holes.
Tunnelled
or non-tunnelled catheter?
A
non-tunnelled catheters provides the easiest and quickest
access to the patient's bloodstream, but its use should
be restricted to the first 1 or 2 weeks of haemodialysis.
Prolonged use
is associated with a high risk of catheter-associated bacteraemia
and central venous obstruction. A
tunnelled catheter is believed to be less prone to infectious complications
Which
central vein?
Subclavian
vein:
With subclavian vein cannulation, there is a 10% rate of severe
acute complications such as arterial puncture with hemothorax
and pneumothorax. Also, when the catheter remains in place for
more than 2 or 3 weeks, there is a 4050% risk of
subclavian vein stenosis or occlusion. Therefore, a subclavian
access should not be selected as long as other central
veins can be punctured. Unfortunately, it is commonly seen catheters
placed via the subclavian vein, usually by surgeons. In
interventional radiology practice, the internal jugular vein is
selected for central catheter placement.
Internal jugular vein: This is the
ideal vein for access. It runs straight down to the superior vena
cava, which obviously reduces the risk of malposition of
the catheter and possibly also of central venous obstruction.
External jugular vein:
On both sides this vein opens into the subclavian vein almost
at a right angle, which occasionally complicates implantation
of stiff, central catheter.
This may also provoke subclavian-vein stenosis and
thrombosis.
Common femoral vein:
The frequency of catheter-associated bacteremia is
higher.
Percutaneous
or surgical implantation?
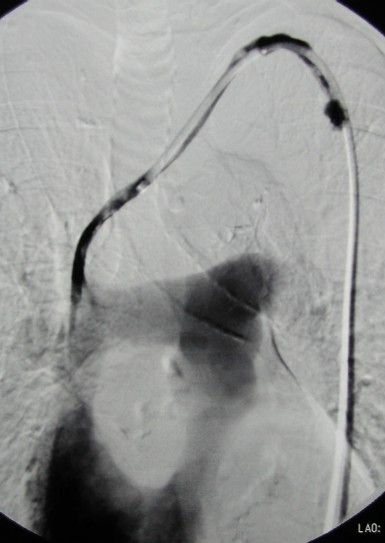
With
ultrasound guidance and X-ray control of the course
of the guide wire and later the position of the catheter
tip (at the SVC/right atrial junction or in the right atrium),
percutaneous implantation can be performed safely and
quickly. Surgical implantation should be considered after
multiple previous cannulations or after neck surgery
(thyroid resection, carotid artery reconstruction, etc.), or
when ultrasound guidance is impossible or has failed.
Complications:
Catheter dysfunction and occlusion:
Primary malposition or later dislocation of the catheter tip will
result in inadequate flow. Interventional repositioning
of the catheter tip or catheter exchange are necessary to
allow for an efficient haemodialysis. Depending on the time of
implantation, partial or complete catheter occlusion
occurs in 3060% of central catheters. A thrombus in the catheter
hub can often be dissolved by local thrombolysis. A
thrombus at the tip of the catheter or a fibrin sheath
around it may resist local thrombolysis. This catheter can then be
stripped off the thrombus using a transfemoral approach. If
this maneuver fails, catheter exchange is usually
necessary. Most interventionists prefer catheter exchange over the
wire directly.
Catheter-associated
bacteremia
Femoral-vein catheters have a higher risk of infection
(and cause catheter-associated bacteraemia earlier) than
subclavian or internal jugular-vein catheters. Multiple-lumen
catheters have a higher risk than single-lumen catheters.
Non-cuffed catheters probably have a higher risk than
cuffed ones. The organisms most frequently isolated during catheter
associated bacteremia are Staphylococcus
aureus and Staphylococcus
epidermidis.
In
the majority of patients manifest catheter associated bacteremia
will not be cured by antibiotics alone. Infected
non-cuffed catheters and cuffed catheters with severe,
recurring, or treatment-resistant infection must be
removed.
Central-venous
obstructions
The frequency of catheter associated central venous stenosis and
occlusion is as high as 4050% after cannulation of the
subclavian vein, and may reach 75% once the subclavian catheter
has been infected. Percutaneous dilatation of the stenosis (with
or without stent implantation) is often successful and provides
satisfying mid-term results.

|
|